South Africa mHealth
Improve linkage to care for tuberculosis patients in South Africa.
Overview
Team
Johns Hopkins School of Nursing
Johns Hopkins Center for Clinical Global Health Education
SA National Health Laboratory Services
Jhpeigo
Engineering Teams (on-site and off-site)
Contribution
Creative Director / Project Design / Product Management / Product Design (UX/UI Design)
(All of the work below is my own unless otherwise noted)
Tuberculosis (TB) is the leading cause of death in South Africa and half of the patients with drug-resistant tuberculosis (MDR-TB) do not return to the clinic for treatment. This exacerbates the issue of drug-resistant tuberculosis bacteria and could potentially lead to a greater crisis.
This project leverages South Africa's National Health Lab Service (NHLS) data to create a system of mobile apps and website interfaces to link patients to care and coordinate treatment initiation.
Partnered with Johns Hopkins School of Nursing, Jhpeigo, the South African National Health Laboratory Services, and the South African national government, emocha offers solution to reduce loss to follow-up. By registering individuals digitally from the moment their specimen is collected, employing Linkage Officers, using automatic SMS services, and empowering medical personnel, the MDR-TB Partnership in South Africa seeks to reduce loss to follow-up and get patients into care within 7 days of diagnosis.
This project is currently under development and not available for public distribution.
Issue
Over 50% of MDR-TB patients are lost to follow-up in South Africa.
It is important to track MDR-TB patients for their personal health and also due to the contagious nature of tuberculosis. They are lost because of one or more of the following reasons:
- NHLS specimen tracking form is incorrectly filled out / not filled out at all (or lost entirely) leading to positive test results but no patients to find. This is mostly due to handwriting errors, demotivated or untrained healthcare workers, and the lack of steady identification factors for people in South Africa (ie. identification number, phone number, address, birthdate).
- Specimens are not correctly stored, resulting in contamination and inconclusive results which delay linkage to care for patients.
- Stigmatized perception of MDR-TB leads to hesitancy of revealing a TB status or seeking treatment.
There was also a 3-year backlog of paper forms that are being manually entered into WAMTECH'S EDR Web (national Electronic Drug Resistant TB Registry).
Concept
emocha provides a tool that is part of a nation-wide systemic shift for MDR-TB management.
How might we provide a tool that retains data integrity, provides test results in a sensitive manner, and above all, reduces loss to follow-up? All of this in an environment that lacks steady power, internet connectivity, and transportation, with users who might speak any one of 11+ languages in South Africa and may or may not be literate.
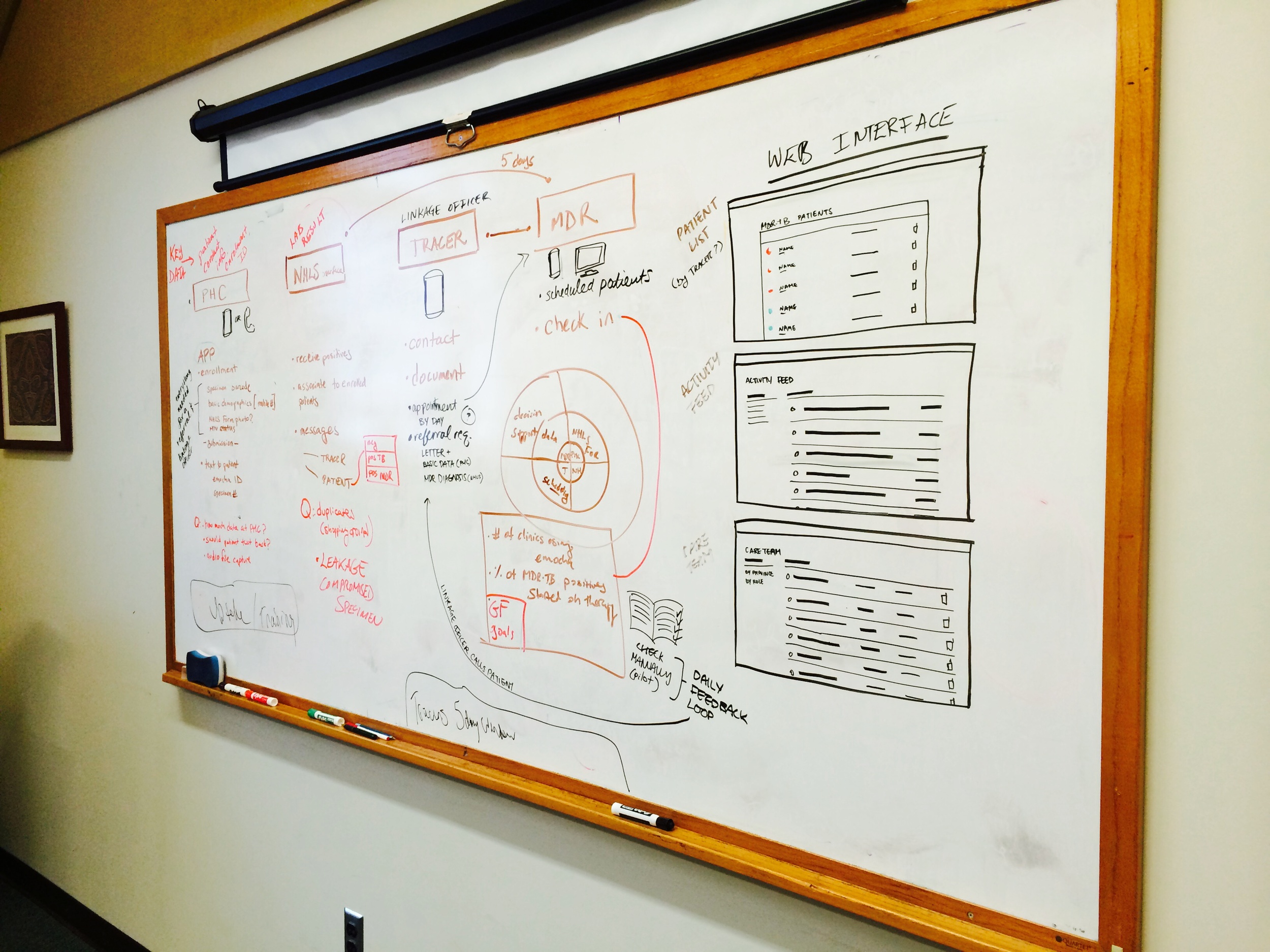
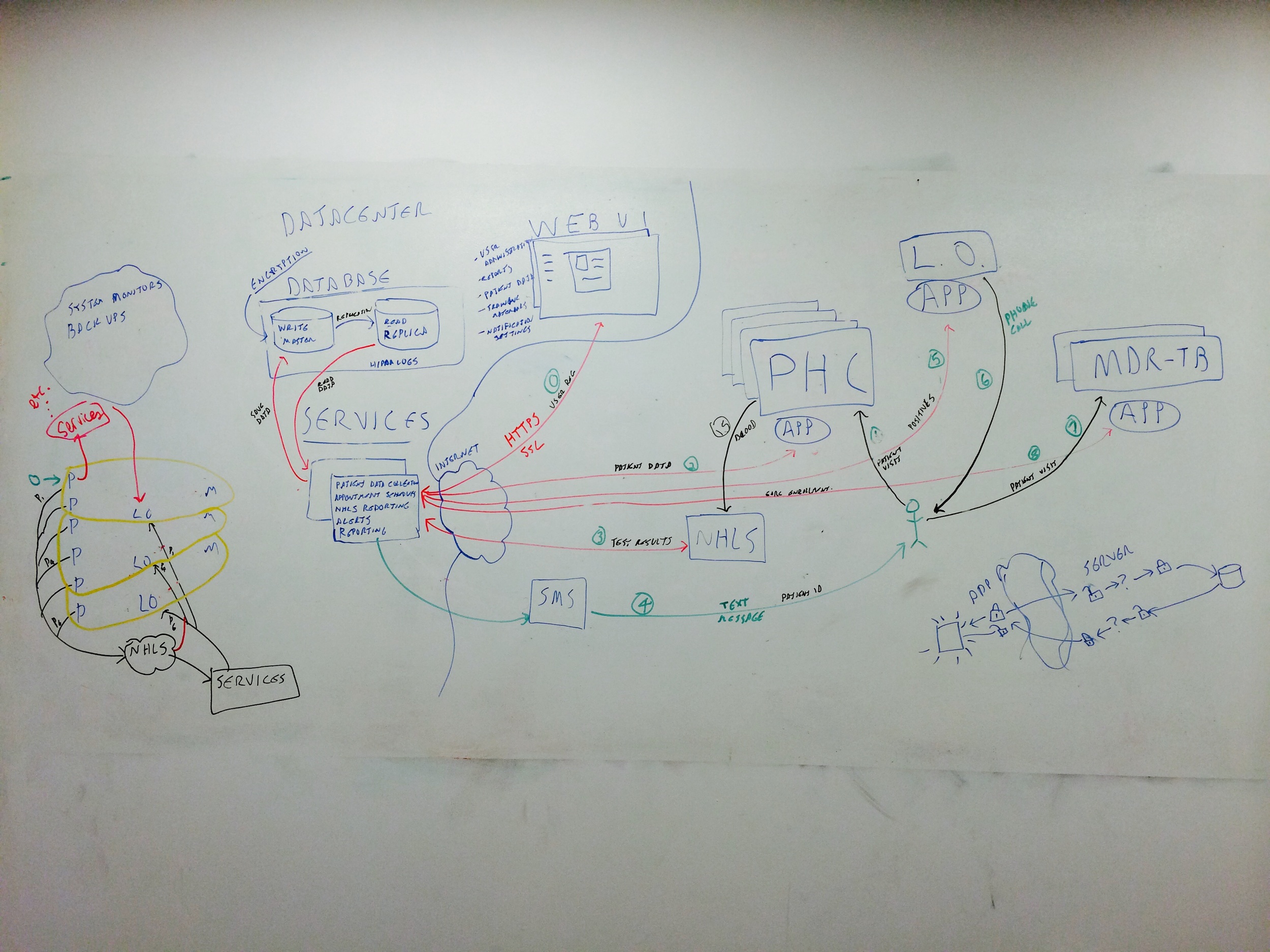
Early whiteboard sessions with clinicians and development teams:
The concept consisted of two parts--
- Mobile Tools
Through mobile tools, we can collect patient health records through digital tools that reduce handwriting errors, missed questions, and lost paper forms. Mobile tools can also use cell-phone reception to transfer data, which is more reliable than internet connectivity. South Africa has a high rate of mobile phone usage, which also allow for automatic SMS reminders and other ways to stay in contact with the patient.
- Training and Education
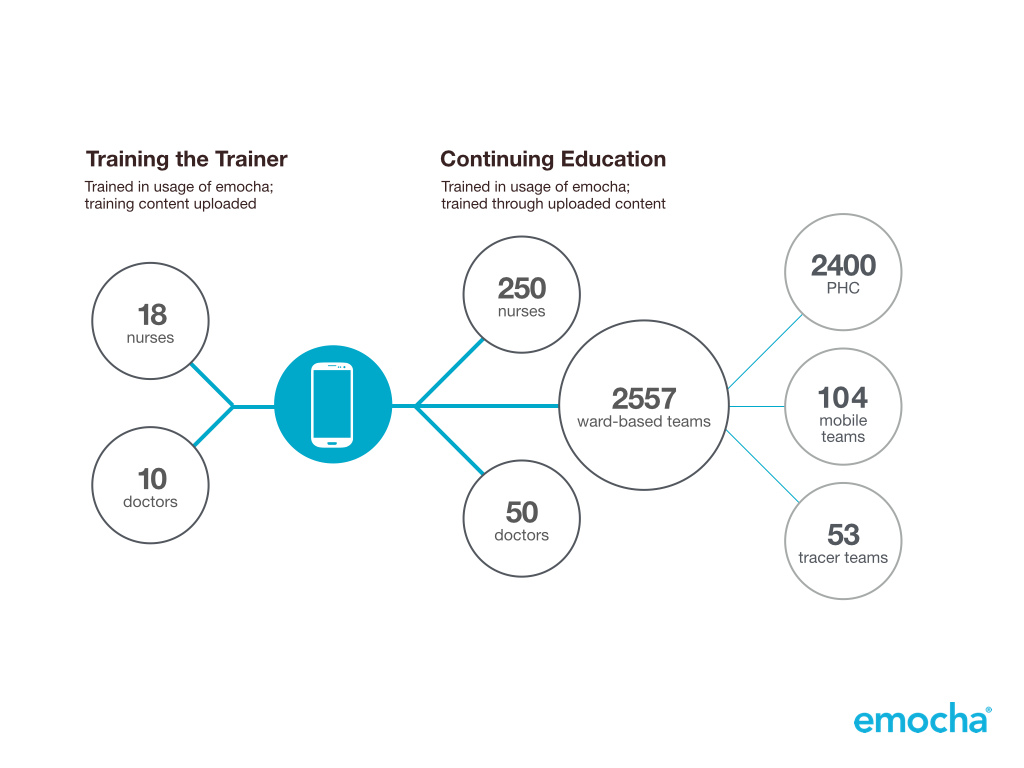
Once again leveraging mobile tools, we can enable country-wide access to videos, documents, and audio training files. Expert clinicians from Johns Hopkins provide training material and best-practice procedures.The scale of the training started with 18 nurses and 10 doctors and would eventually reach approximately 250 nurses, 50 doctors, 2400 primary health clinics, 104 mobile teams, and 53 tracer teams.
Primary Health Clinic – clinics where patients would be tested for TB and potentially hospitalized
Mobile Teams – health clinicians treating TB patients off-site because they did not, or could not show up at the PHC
Tracer Teams – healthcare workers following up with patients who had tested positive and ensure linkage to care
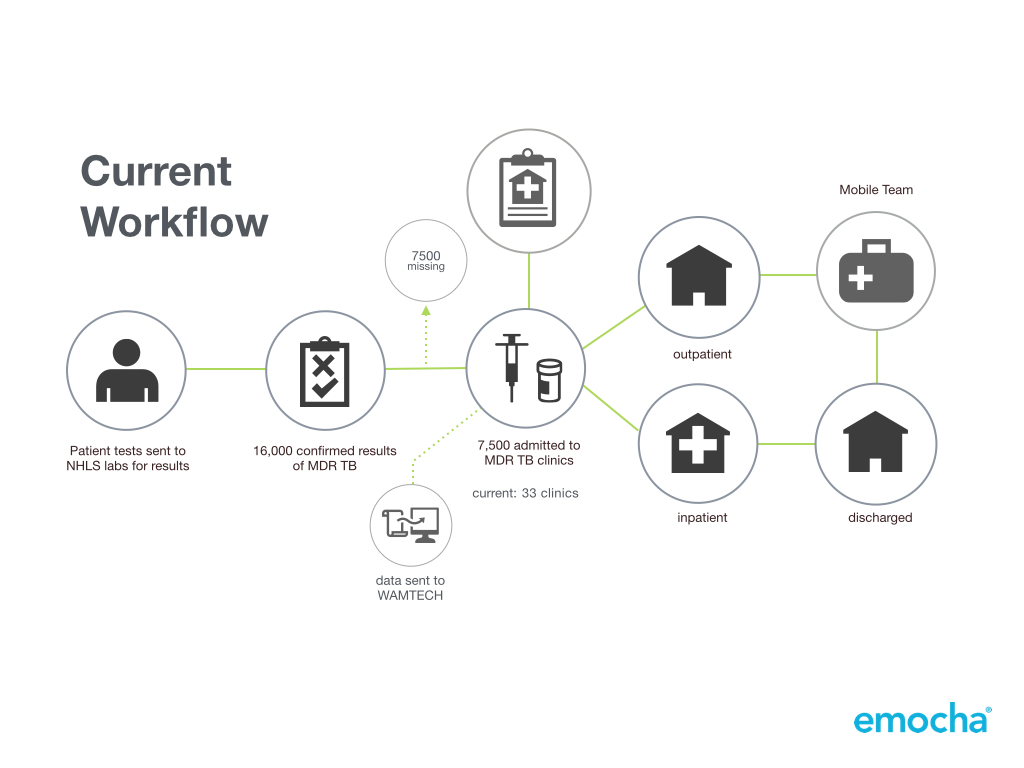
The simplified master workflow showed how the patient moved through the major steps of the process.

In order to achieve this, emocha had to create three separate workflows for the major stakeholders and integrate each of them into the patient's master journey. This consisted of three apps (Primary Health Clinic, Linkage Officer, and MDR-TB Clinic), an SMS messaging system, and a web interface for project management.


Apps
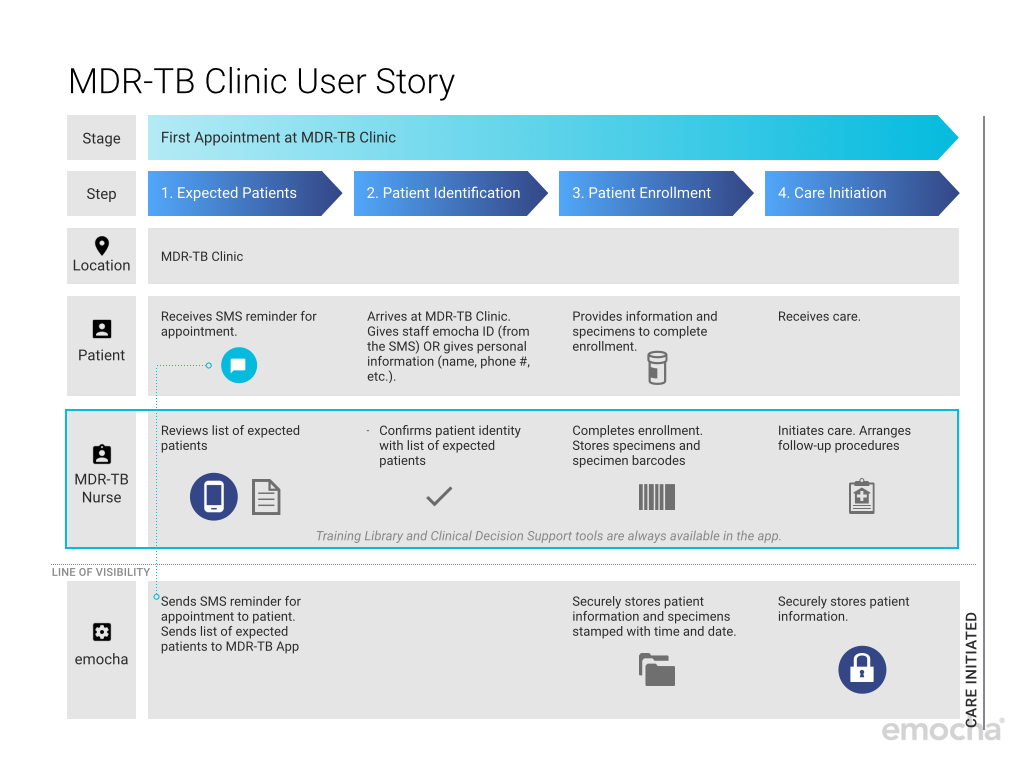
The blueprint below defines key stages for linkage to care and the core tasks that emocha's digital tools conduct behind-the-scenes. It also shows the three apps that are used by nurses at the clinic, linkage officers in the field, and nurses initiating treatment.


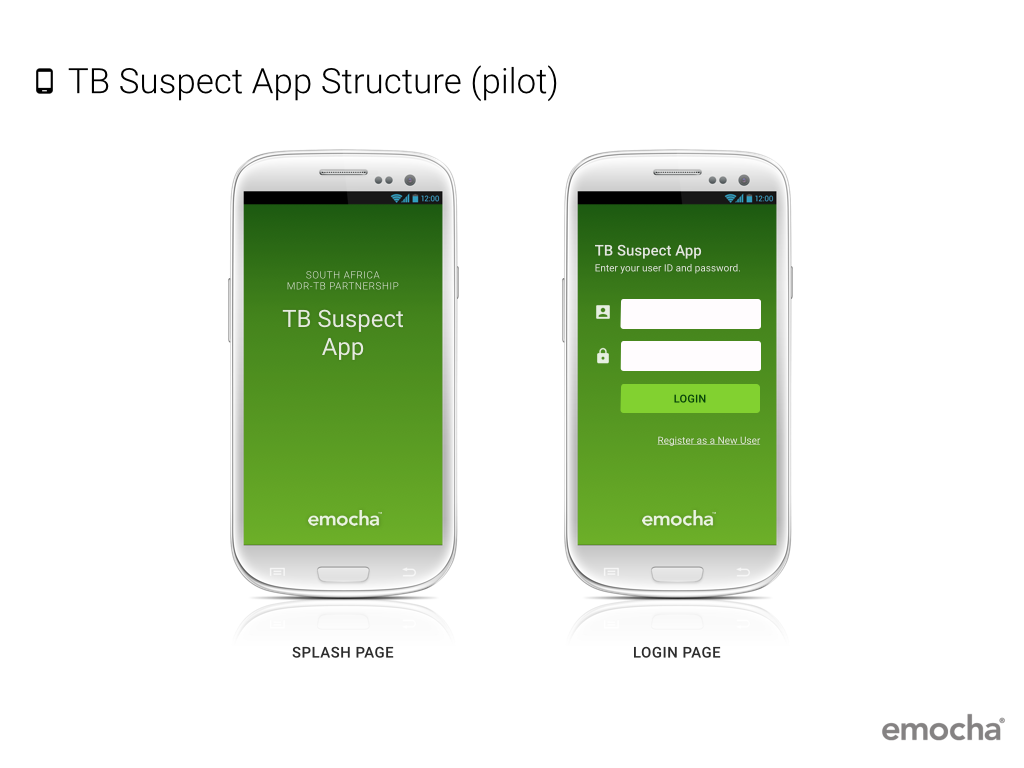
TB Suspect App
Linkage Officer App

MDR-TB Clinic App
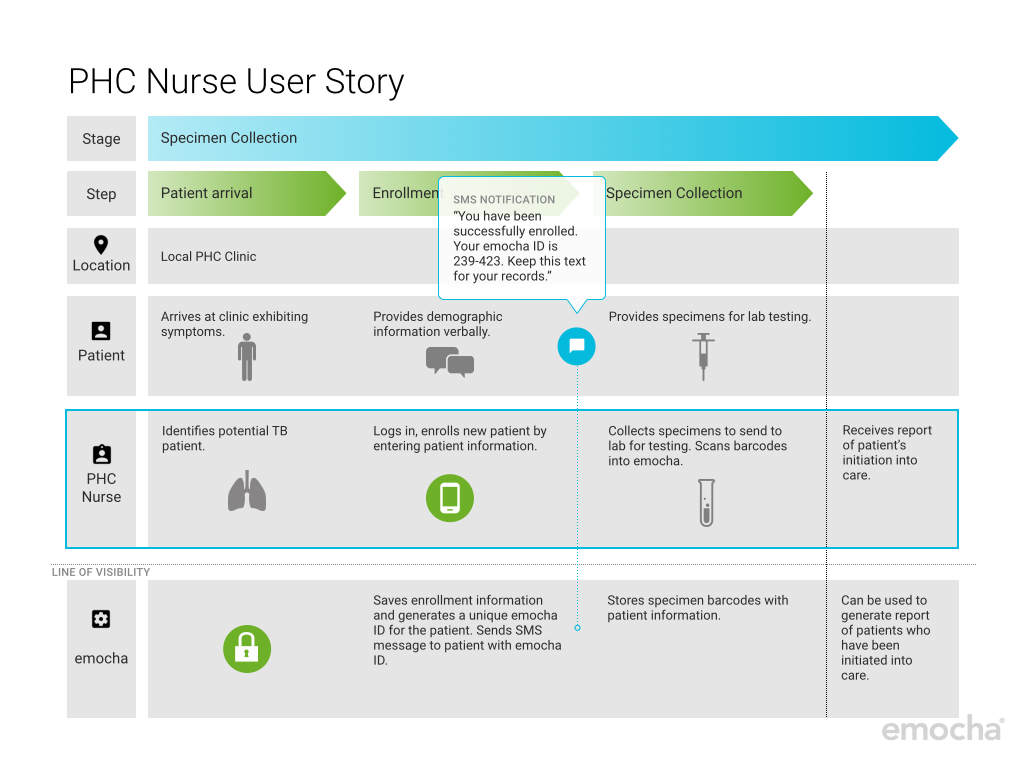
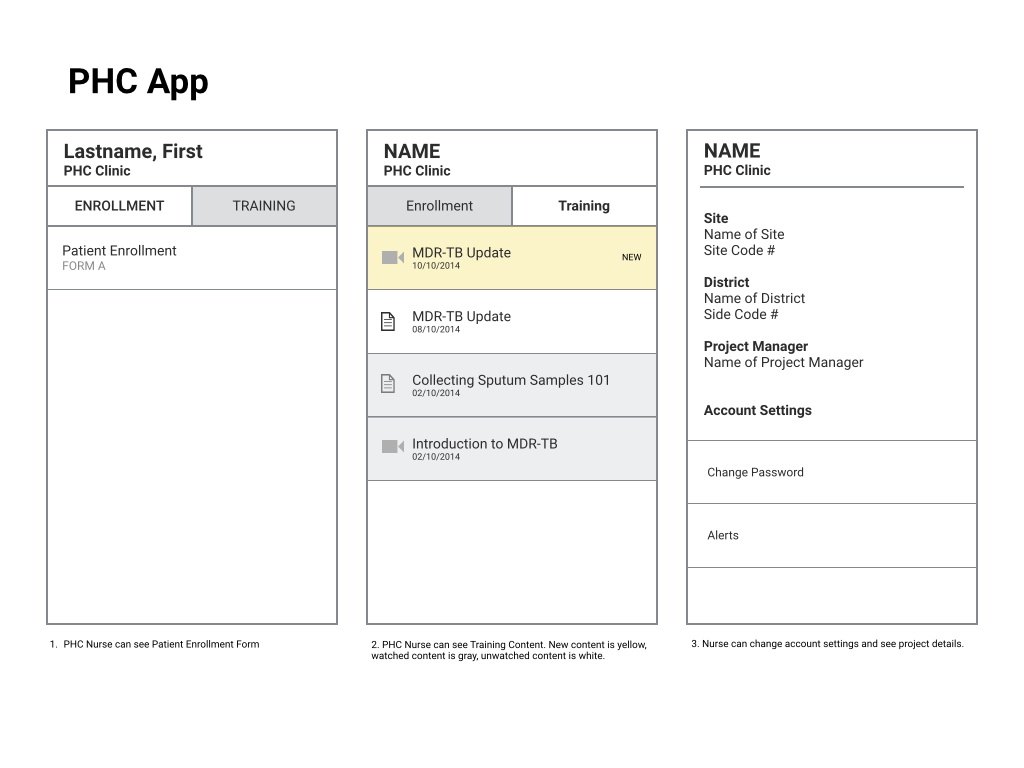
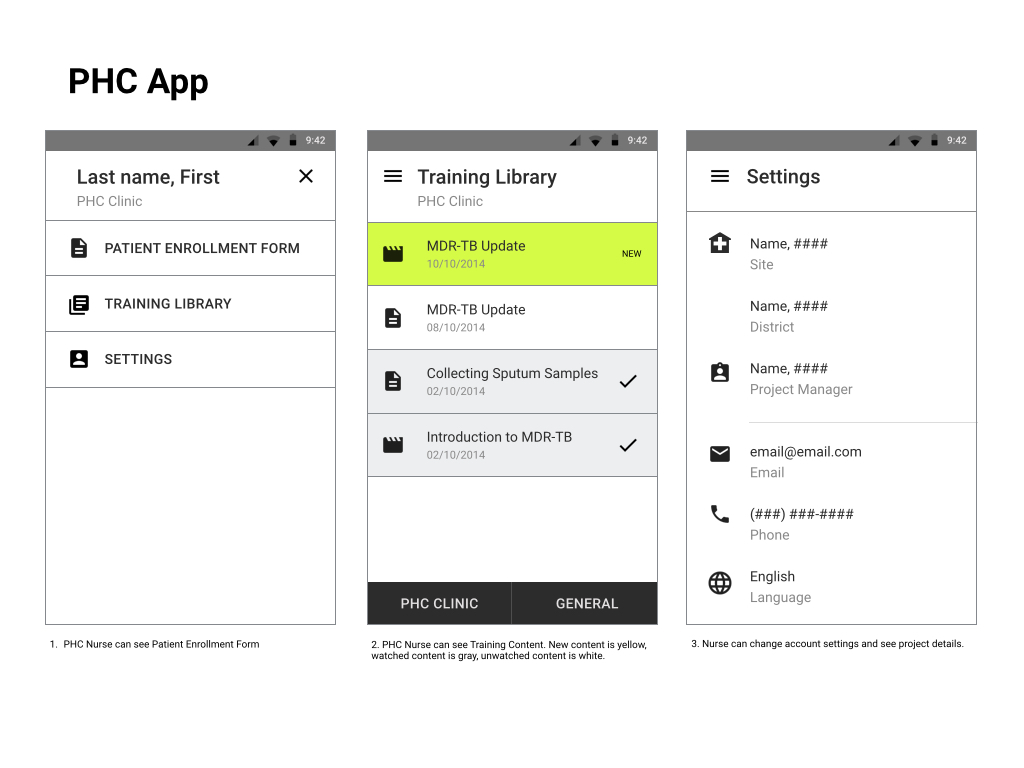
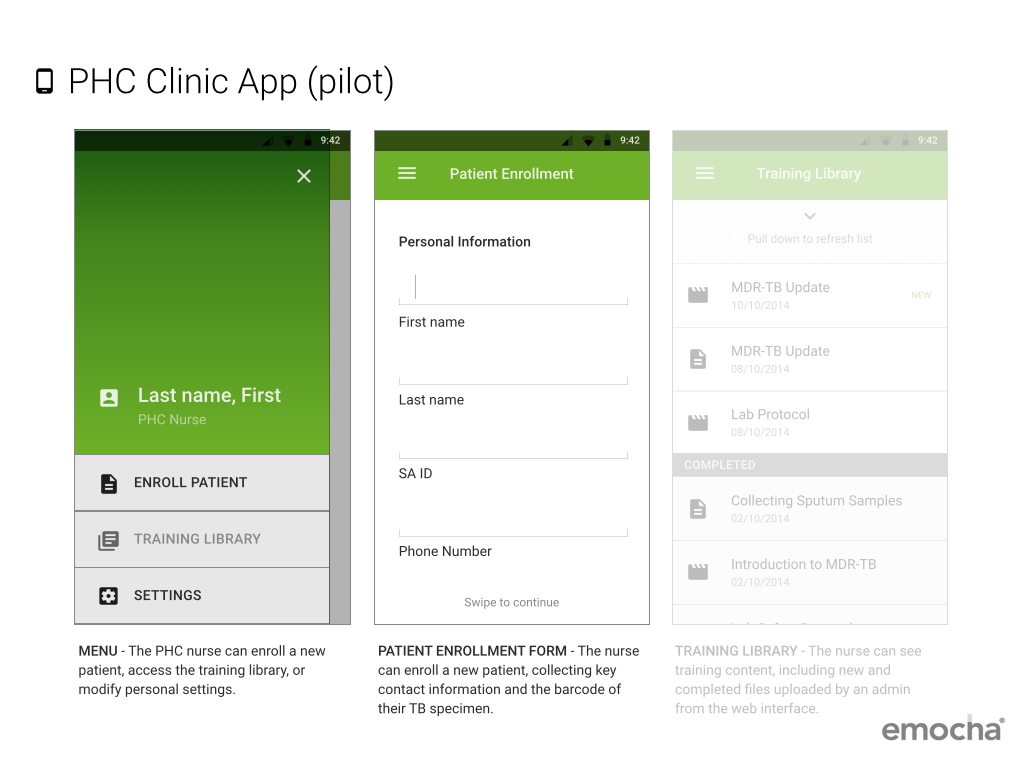
TB Suspect App
This is where specimens are collected and potential patients will be enrolled into emocha. Barcodes for specimens and other identifiers are storied in the emocha database. (User story below made by design intern, Kajsa Nichols-Smith)
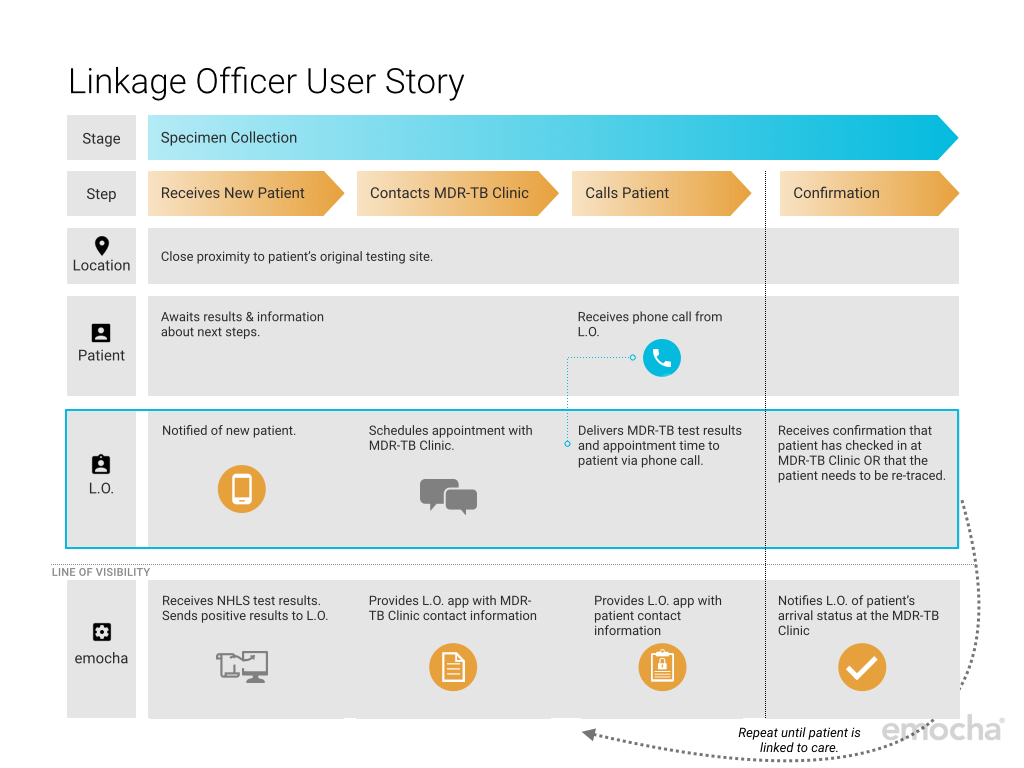
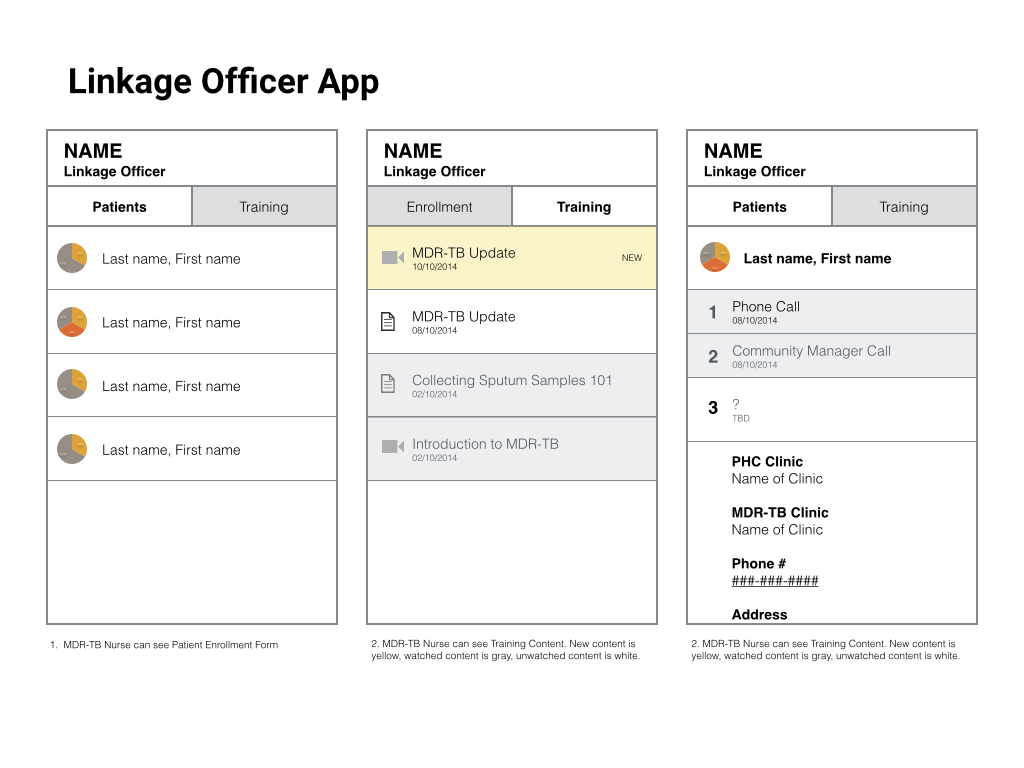
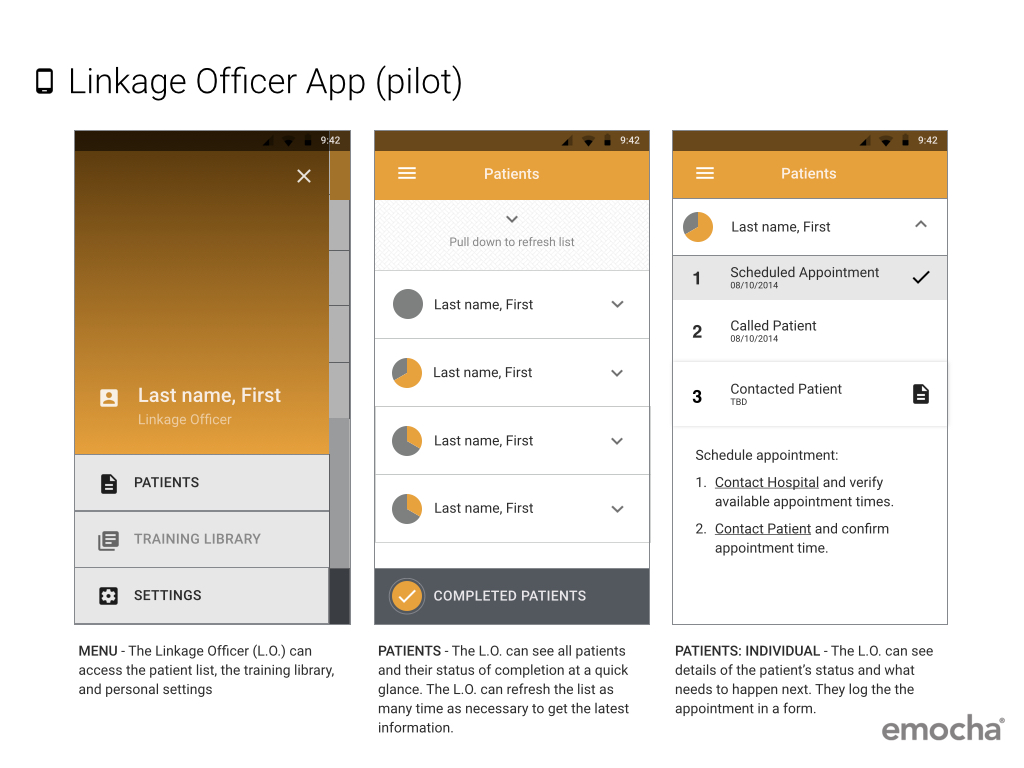
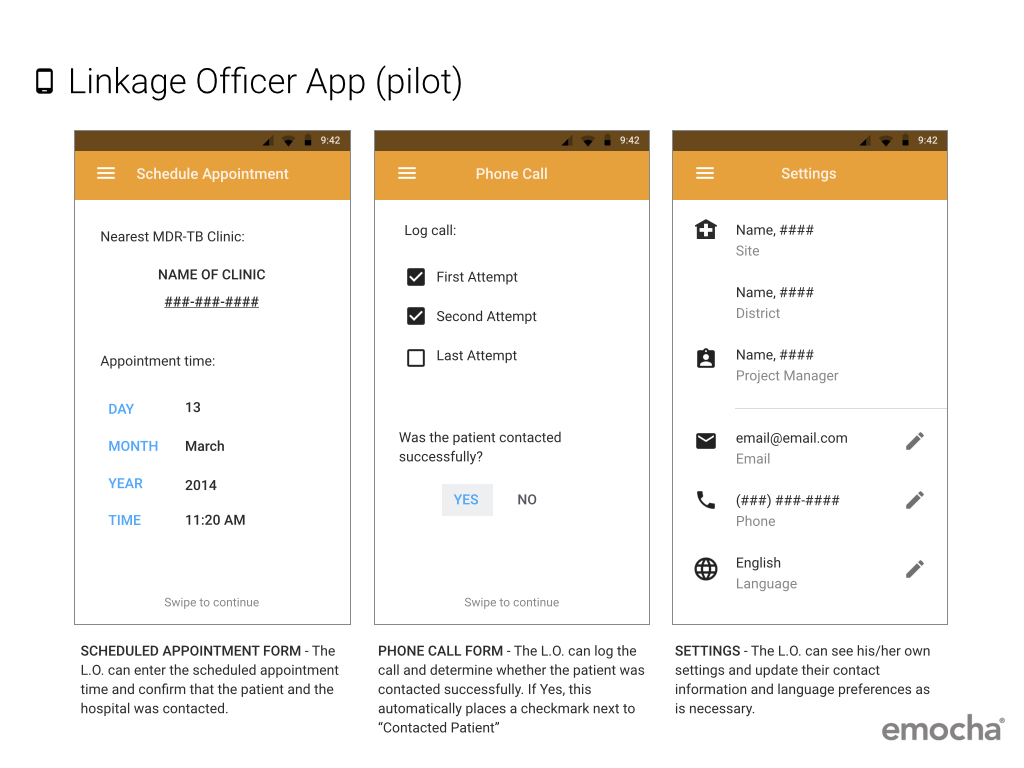
Linkage Officer App
The Linkage Officer is paired with an MDR-TB clinic and all individuals with a positive MDR-TB result in his/her vicinity is sent to the app. From there, they are on a mission to schedule an appointment at the clinic, find the patient, and get them to the clinic within 5 days. (User story below made by design intern, Kajsa Nichols-Smith)

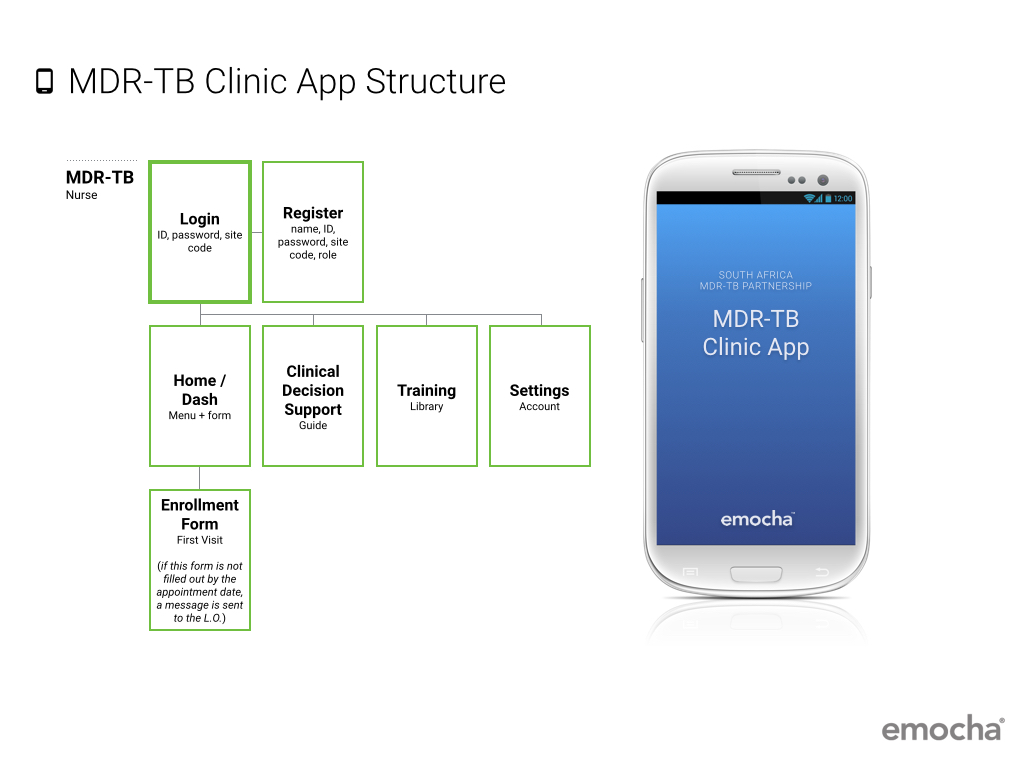
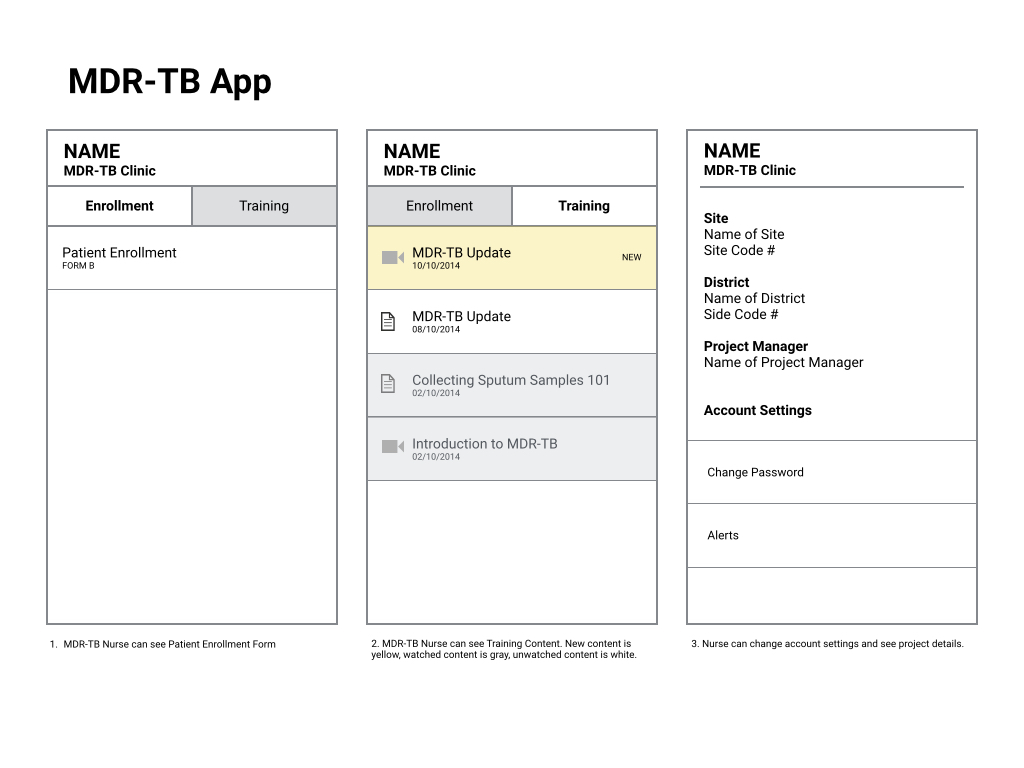
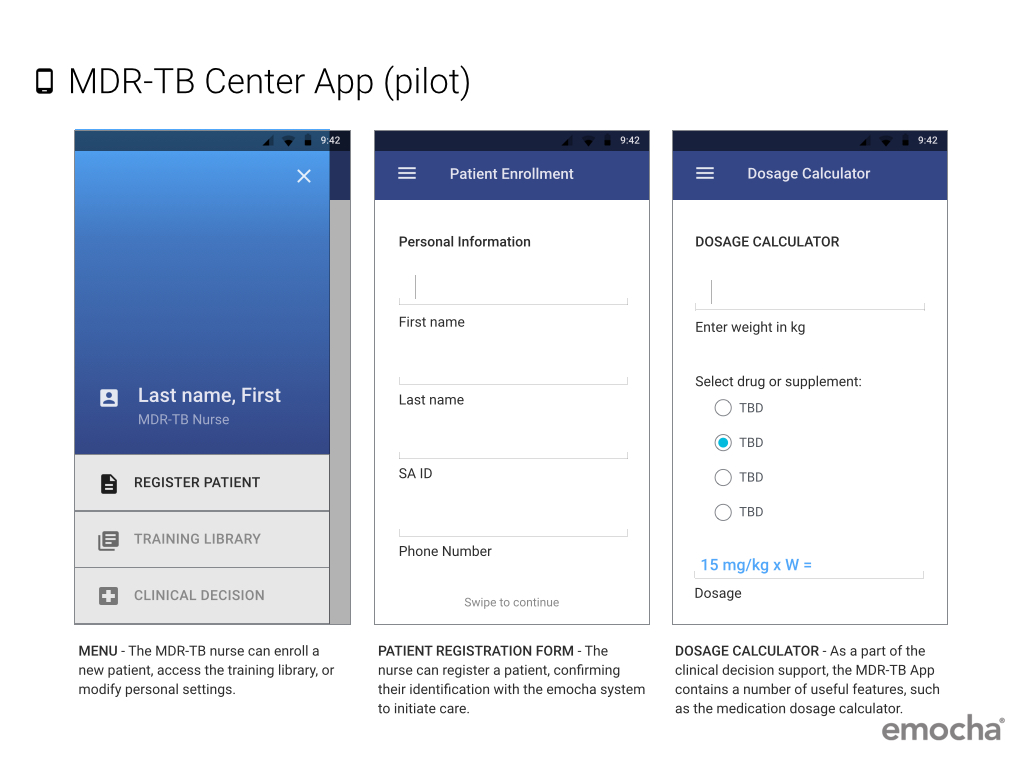
MDR-TB Clinic App
The MDR-TB Clinic can check in a new patient and log them in the system. The app lets them know who to expect, and when. If the patient doesn't show up, they can send a message back to the Linkage Officer who tries to find the patient again.
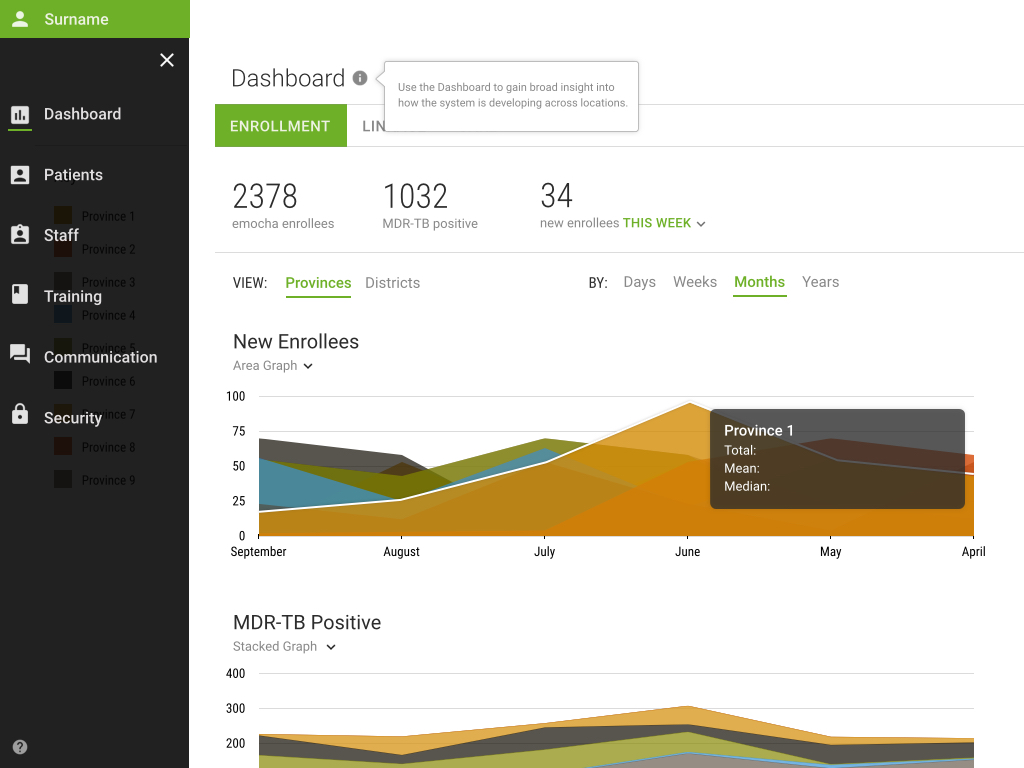
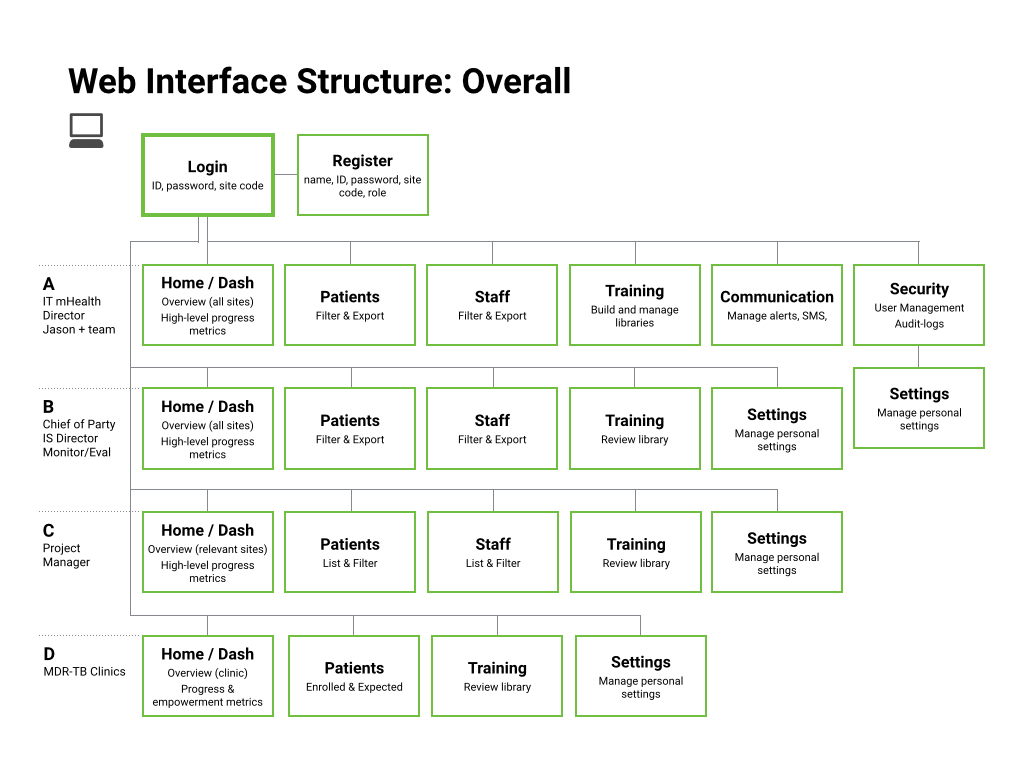
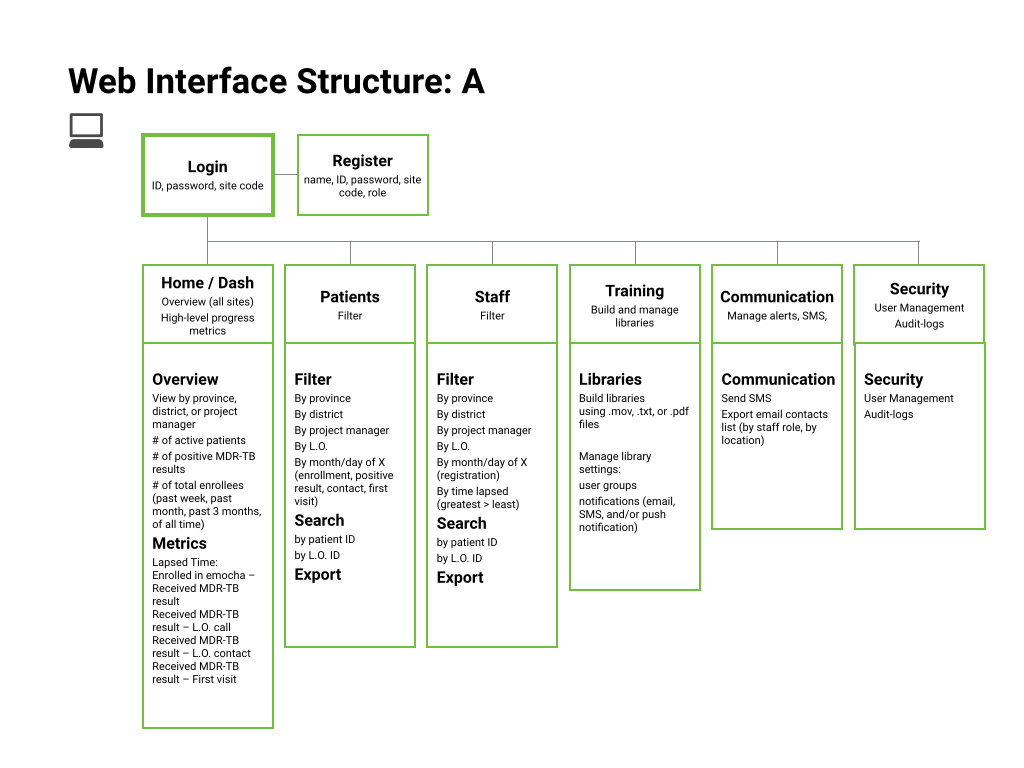
Web App
The web interface is for coordinators, directors, clinicians, and project managers to monitor the different aspects of the project. Through the metrics the managers could observe locations that required extra attention, make critical adjustments to improve linkage outcomes, and report any changing trends at a district, province, or national level.

Timeline
The apps were pilot-tested in 2015 and a phased roll-out began in 2016. This tool is used in South Africa today.

Image courtesy of emocha.com
This project remains underdevelopment and is not intended for public distribution.